
Innovation in Women's Health
Innovation in Women's Health
Welcome to Tech for All’s substack that explores how innovators and entrepreneurs are using technology to innovate for historically underserved groups, and the barriers that hinder progress.


An explosion of much-needed coverage on menopause last week discussed the mental and physical effects of menopause, as well as the challenges that women face in getting treatment or even raising the issue in the workplace.1 The historical lack of attention on menopause by doctors and researchers has likely led to women receiving poorly-informed medical advice, though that is starting to change with platforms like Elektra, a healthcare company focused on providing menopause education and care through expert coaching and community support.2 And to stress the point, this is about a common issue: 75% of women who reach menopause experience symptoms. Why the seeming underprovision of menopause-related innovation?
One reason is simple: the people most likely to experience menopause (women) have historically been excluded from becoming inventors and entrepreneurs.3 As a result, the women who do end up becoming inventors tend to be exceptional in that they identified problems the medical establishment had ignored, and they overcame gendered barriers in their careers. Take Geetha Manjunath, who built a startup in India, Niramai, using artificial intelligence and machine learning to make thermal imaging a touch-free, radiation-free means for early detection of breast cancer. Uniquely situated for the task, Dr. Manjunath is a woman with a PhD in computer science from the Indian Institute of Science, extensive experience in AI and ML, and a network of experts in different fields—including one friend who pointed her to thermal imaging as an avenue to explore for breast cancer detection. But it was a personal trauma that prompted her to quit her high profile job in 2017 and devote her career to improving breast cancer diagnosis using AI-based thermal imaging: she had lost two close family members to the disease.4 If any one of the coincidences that led Dr. Manjunath to do this work didn’t happen—the loss in her family, holding a PhD, leading research at a lab—it’s entirely possible this technology wouldn’t exist, because there are only a handful of women who have the necessary training to apply AI to thermal imaging.
Another example is Linda Griffith, who opened in 2009 the Center for Gynepathology Research at MIT, where she is a professor of biological and mechanical engineering. The center is the only engineering lab in the United States to focus on endometriosis, a disease affecting 10% of women—or anyone who menstruates—causing tissue to grow outside the uterus, which results in severe pain and, in some cases, infertility. Having watched her niece suffer from the same disease that Dr. Griffith herself had, her mission to tackle this poorly understood disorder was deeply personal. And it wasn’t only this personal experience combined with her professional position that uniquely qualified her for the task: she had also been awarded $.5M for a research project of her choosing as part of the MacArthur “genius” grant. Few researchers receive a grant of this scale without limitations on projects to which it can be applied. Dr. Griffith’s pioneering research on endometriosis, then, was only possible through a series of coincidences. The fact that it takes a genius to open this lab illustrates the lack of interest in this space, where the bar is significantly higher. If Dr. Griffith didn’t get the grant, have the scientific background, or have a personal interest in a disease that hit both her niece and herself, it is all too easy to imagine that there would be no engineering lab focused on endometriosis anywhere in the US.
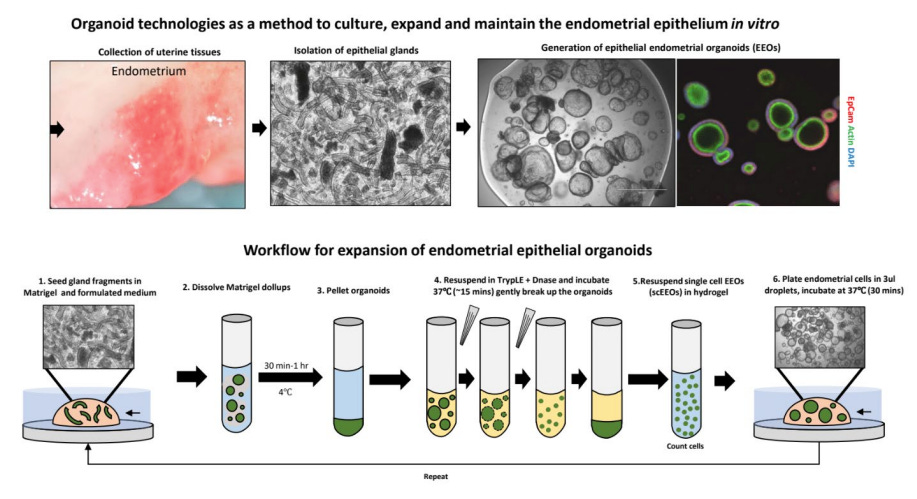
A sketch from the MIT Center for Gynepathology Research illustrating the process of creating endometrial epithelial organoids for patient avatars, part of the research done by Dr. Griffith and her team.
A second obstacle complicates work on women’s health even more. While we’ve begun to rid ourselves of the long-held notion that women’s “proper” role is limited to the home, our perception around the menstrual cycle is not keeping up. And as it remains a social taboo around the world, a host of menstruation-related issues suffer from a stigma that renders them hard to talk about—and hard to invent around, much like menopause. Having suffered from endometriosis for decades and pioneered research to understand the disease, Dr. Griffith was diagnosed with breast cancer and noticed the overwhelming differences in research as well as society’s perception of and reaction to the disease. Dr. Griffith called her stage 2 breast cancer a “stormy-day walk in the park” compared to her endometriosis. Yet the medical treatment that she got for breast cancer, combined with the sympathy and help from those around her, left her baffled. Even though breast cancer is specific to women, its status both within and outside healthcare is that of any cancer or other commonplace diseases, not of a women’s disease.
Dr. Manjunath began her journey by talking with her colleagues to better understand the problem. One was an imaging expert in Palo Alto, who pointed her to thermal imaging. “So I read the papers on that,” she recalled, “and that is how my interest in thermal imaging started.”5 Had she been interested in working on another women’s health issue, would it have gone this smoothly? Would she have been able to learn from one of her colleagues just the direction that would be most useful for her to investigate? Would she have found papers on the topic as a starting point on which she could build her research?
In fact, Ridhi Tariyal, who completed her graduate education and worked at Harvard and MIT, has experienced this exact problem. Like Dr. Manjunath, Tariyal brought her background as a scientist to a women’s health startup that she co-founded, NextGen Jane. But as opposed to Dr. Manjunath’s focus on breast cancer, Tariyal set out to pitch an idea that even women called “gross”: using a smart tampon to collect women’s menstrual blood as a window to their reproductive health. She quickly realized, though, that menstrual issues seem to be a taboo in a way that breast cancer is not. When Tariyal and her co-founder began considering women’s menstrual blood as a means to get information about their health, they thought of it as “an asset that surely someone’s looked into,” but quickly learned that was not the case. “No one had looked into it . . . It was shocking. Now there are people who are beginning to investigate it,” Tariyal explained, “but when we started down this journey a decade ago, papers in this area were really scarce.” Often, they’ve received negative feedback for using menstrual blood.
“We started out thinking that we wanted to do STI tracking. And the resistance that idea met was almost universal, show stopping to the extent that we dropped the idea. We spoke to the best STI academic lab in the country at the time, and it was run by women, so I thought they’d get it immediately. And they said: Can we give you a piece of advice? You need to lose the menstrual portion of this entire idea. No lab in America wants to work with menstrual blood.” — Ridhi Tariyal
The gaps between different taboos in different places present another barrier. India, Dr. Manjunath’s home country, is one example of a place where social norms make the touch-free element of her solution an asset, as many women prefer to avoid an examiner touching their breasts. Tariyal too received requests from researchers in India and several countries in Africa, where “most doctors are male, and women would rather use a tampon than have a male doctor look down there.” Tariyal had already seen the impact of a lack of understanding of different social dynamics in 2012, in her first attempt to launch a startup—a genomics application targeted towards the Indian market and designed to test the blood of couples in arranged marriages for genetic disorders that their potential children might inherit. “Trying to explain to people in the US how there is a vibrant middle class in India that is willing to pay for genomics products was difficult.”
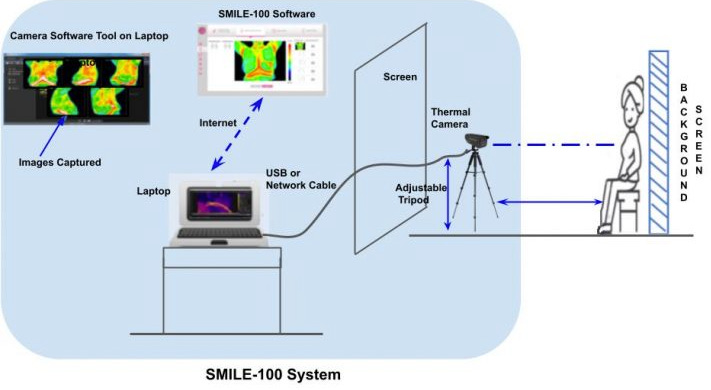
A sketch of Niramai’s SMILE-100 System, which traces the screening process from taking the pictures in a private setting to analyzing them using the AI algorithm, one of the products created by Dr. Manjunath and her team.
Taken together, the stories of Dr. Manjunath, Dr. Griffith, and Tariyal offer a glimpse into women’s health as a gateway to the sociological barriers that limit the application of technology. These barriers are at the heart of our work at the Tech for All lab, and they apply beyond just women’s health. For example, it has been established that talented individuals from the global south are orders of magnitude less likely to become inventors. One study found that International Mathematical Olympiad participants from low-income countries produce 34 percent fewer scientific publications and 56 percent fewer citations than equally talented rich-country counterparts.6 Does this gap cause science to focus less on the needs of those in the global south? Similarly, a study of the US concluded that children from families in the the top 1 percent of the income distribution are 10 times as likely to have filed for a patent as those from below-median-income families, and white children are three times as likely to have filed a patent as black children, resulting in millions of people who might have become inventors had they come from different backgrounds.7 Again, does this lead to fewer inventions for both black and lower-income Americans? And social norms also limit the application of technology beyond gender. A recent study of rural India documents that workers are less likely to do tasks that are associated with lower ranked castes. Do these norms then lead to fewer products serving people in “untouchable” castes?
More importantly, beyond just identifying these gaps and biases when it comes to innovation, how might we broaden the use of technology to serve the needs of a greater number of people of different genders, races, countries, and socioeconomic backgrounds? Sign up for our substack for future posts on the opportunities we miss, and how we can make innovation and entrepreneurships more inclusive.
Co-founded by Alessandra Henderson and Jannine Versi, MIT and Harvard Business School alumni.
Koning, Rembrand, Sampsa Samila, and John-Paul Ferguson. “Who Do We Invent for? Patents by Women Focus More on Women’s Health, but Few Women Get to Invent.” Science 372, no. 6548 (June 2021): 1345–1348; Koning, Rembrand, Sampsa Samila, and John-Paul Ferguson. “Inventor Gender and the Direction of Invention.” AEA Papers and Proceedings 110 (May 2020): 250–254. Koning et al. show that a lack of representation among inventors translates into a lack of breadth in inventions. Biomedical patents invented by all-female teams are 35% more likely than all-male teams to focus on women’s health, but only 4% of female-focused patents are from all-female teams.
Both of them were young and got mammograms, but mammography could only detect their breast cancer when it was too progressed to save them. And they were not an exception: mammography is ineffective for early-stage detection of breast cancer below the age of 40 or 50, when women tend to have dense breasts (breasts with more fibro-glandular tissue).
For early work on thermal imaging and breast cancer, see for example, M. Kontos, R. Wilson, I. Fentiman, “Digital infrared thermal imaging (DITI) of breast lesions: sensitivity and specificity of detection of primary breast cancers.” Clinical Radiology, Volume 66, Issue 6, 2011, Pages 536-539; Nimmi Arora, Diana Martins, Danielle Ruggerio, Eleni Tousimis, Alexander J. Swistel, Michael P. Osborne, Rache M. Simmons, “Effectiveness of a noninvasive digital infrared thermal imaging system in the detection of breast cancer.” The American Journal of Surgery, Volume 196, Issue 4, 2008, Pages 523-526. For more recent work, see for example Kandlikar S., Perez-Raya I., Raghupathi P.G., Hernandez J.L., Dabydeen D., Medeiros L., Phatak P., “Infrared imaging technology for breast cancer detection – Current status, protocols and new directions.” International Journal of Heat and Mass Transfer 108: 2303–2320, 2017.
Agarwal, Ruchir, and Patrick Gaule. “Invisible Geniuses: Could the Knowledge Frontier Advance Faster?” American Economic Review: Insights 2, no. 4 (Dec 2020): 409-24.
Bell, Alex, Raj Chetty, Xavier Jaravel, Neviana Petkova, and John Van Reenen. “Who Becomes an Inventor in America? The Importance of Exposure to Innovation.” Quarterly Journal of Economics 134, no. 2 (2019): 647-713.